"Purchase asacol online, symptoms bipolar disorder".
By: N. Taklar, M.B.A., M.B.B.S., M.H.S.
Assistant Professor, University of Central Florida College of Medicine
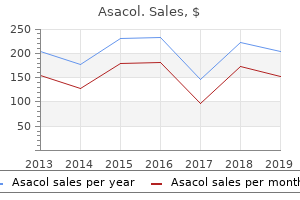
Conversely anima sound medicine asacol 800 mg on-line, tetraethylammonium ions block K+ currents without affecting Na+ currents medicine you can take during pregnancy buy asacol now. The differential sensitivity of Na+ and K+ currents to these drugs provides strong additional evidence that Na+ and K+ flow through independent permeability pathways treatment for uti buy asacol 400mg cheap. As discussed in Chapter 4 medications for osteoporosis order asacol mastercard, it is now known that these pathways are ion channels that are selectively permeable to either Na+ or K+. In fact, tetrodotoxin, tetraethylammonium, and other drugs that interact with spe- + + 460 mM Na+ 0 Early current is inward Membrane current (mA/cm2) -1 +1 Na+-free 0 Early current is outward -1 +1 460 mM Na+ 0 Early current is inward again -1 0 2 4 Time (ms) 6 8 52 Chapter Three Figure 3. Panel (1) shows the current that flows when the membrane potential of a squid axon is depolarized to 0 mV in control conditions. Two Voltage-Dependent Membrane Conductances the next goal Hodgkin and Huxley set for themselves was to describe Na+ and K+ permeability changes mathematically. To do this, they assumed that the ionic currents are due to a change in membrane conductance, defined as the reciprocal of the membrane resistance. Membrane conductance is thus closely related, although not identical, to membrane permeability. When evaluating ionic movements from an electrical standpoint, it is convenient to describe them in terms of ionic conductances rather than ionic permeabilities. The difference between Vm and Eion is the electrochemical driving force acting on the ion. Hodgkin and Huxley used this simple relationship to calculate the dependence of Na+ and K+ conductances on time and membrane potential. From these measurements, Hodgkin and Huxley were able to calculate gNa and gK (Figure 3. For example, both Na+ and K+ conductances require some time to activate, or turn on. In particular, the K+ conductance has a pronounced delay, requiring several milliseconds to reach its maximum (Figure 3. The more rapid activation of the Na+ conductance allows the resulting inward Na+ current to precede the delayed outward K+ current (see Figure 3. Although the Na+ conductance rises rapidly, it quickly declines, even though the membrane potential is kept at a depolarized level. This fact shows that depolarization not only causes the Na+ conductance to activate, but also causes it to decrease over time, or inactivate. The K+ conductance of the squid axon does not inactivate in this way; thus, while the Na+ and K+ conductances share the property of time-dependent activation, only the Na+ conductance inactivates. Depolarizations to various membrane potentials (A) elicit different membrane currents (B). Below are shown the Na+ (C) and K+ (D) conductances calculated from these currents. Both peak Na+ conductance and steady-state K+ conductance increase as the membrane potential becomes more positive. In addition, the activation of both conductances, as well as the rate of inactivation of the Na+ conductance, occur more rapidly with larger depolarizations. The peak magnitude of Na+ conductance and steady-state value of K+ conductance both increase steeply as the membrane potential is depolarized. This finding accounts for more rapid time courses of membrane currents measured at more depolarized potentials. Note the similar voltage dependence for each conductance; both conductances are quite small at negative potentials, maximal at very positive potentials, and exquisitely dependent on membrane voltage at intermediate potentials. The observation that these conductances are sensitive to changes in membrane potential shows that the mechanism underlying the conductances somehow "senses" the voltage across the membrane. All told, the voltage clamp experiments carried out by Hodgkin and Huxley showed that the ionic currents that flow when the neuronal membrane is depolarized are due to three different voltage-sensitive processes: (1) activation of Na+ conductance, (2) activation of K+ conductance, and (3) inactivation of Na+ conductance. Reconstruction of the Action Potential From their experimental measurements, Hodgkin and Huxley were able to construct a detailed mathematical model of the Na+ and K+ conductance changes. The goal of these modeling efforts was to determine whether the Na+ and K+ conductances alone are sufficient to produce an action potential. Using this information, they could in fact generate the form and time course of the action potential with remarkable accuracy (Figure 3.
Interactive effects of fitness and duration of hormone treatment on prefrontal cortex volume and executive function medicine man movie discount asacol 400mg on line. Cerebral glucose metabolism in adolescent girls with attention-deficit/hyperactivity disorder symptoms yeast infection purchase 800 mg asacol overnight delivery. Cerebral glucose metabolism in adolescent girls with attention-deficit/hyperctivity disorder symptoms walking pneumonia discount asacol express. Conjugated equine estrogens and global cognitive function in postmenopausal women treatment episode data set purchase genuine asacol on-line. Visual agnosia: Disorders of object vision and what they tell us about normal vision. Visuospatial cognition in Williams syndrome: Reviewing and accounting for the strengths and weaknesses in performance. Wisconsin Card Sorting Test and Halstead Category Test performances of children and adolescents who exhibit the syndrome of nonverbal learning disabilities. Regional cerebral blood flow correlates of language processes in reading disability. The impact of childhood hypothalamic/ chiasmatic brain tumors on child adjustment and family functioning. Epidemiological surveys of autism and other pervasive developmental disorders: An update. The utility of math difficulties, internalized psychopathology, and visual-spatial deficits to identify children with nonverbal learning disability syndrome: Evidence for a visual-spatial disability. Transmissible and non-transmissible amyloidoses: Autocatalytic post-translational conversion of host precursor proteins to beta-pleated configuration. Effect of varying conditions of fear on immobility reactions in domestic chickens (Gallus gallus). Functional magnetic resonance imaging of visual object construction and shape discrimination: Relations among task, hemispheric lateralization, and gender. Quantitative morphology of the corpus callosum in attention deficit hyperactivity disorder. The constraints functional neuroimaging places on classical models of auditory word processing. A large-scale distributed network for covert spatial attention: Further anatomical delineation based on stringent behavioural and cognitive controls. Dynamic mapping of human cortical development during childhood through early adulthood. Neuronal production, migration, and differentiation in a vocal control nucleus of the adult female canary brain. Circuitry of primate prefrontal cortex and representation of behavior by representational memory. Topography of cognition: Parallel distributed networks in primary association cortex. Cerebral asymmetry and the effects of sex and handedness on brain structure: A voxel-based morphometric analysis of 465 normal adult human brains. A behavioral analysis of degree of reinforcement and ease of shifting two new responses in a Weigl-type card sorting problem. Susceptibility loci for distinct components of developmental dyslexia on chromosome 6 and 15. Brain activation during human navigation: Gender-different neural networks as substrate of performance. Sex and handedness differences in cerebral blood flow during rest and cognitive activity. Sex differences in brain gray and white matter in healthy young adults: Correlations with cognitive performance. Social and emotional responsivity of children with nonverbal learning disabilities. Dissertation Abstracts International: Section B: the Science and Engineering, 57, 6573. Mental phenomena evoked by electrical stimulation of the human hippocampal formation and amygdala.
The tetanizing stimulation causes Ca 2+ to accumulate in the presynaptic neuron to such a degree that the intracellular binding sites that keep cytoplasmic Ca2+ low are overwhelmed treatment kawasaki disease generic 400mg asacol. Habituation When a stimulus is benign and is repeated over and over medicine website generic asacol 800 mg without prescription, the response to the stimulus gradually disappears (habituation) medicine 94 buy asacol online. This is associated with de-creased release of neurotransmitter from the presynaptic terminal because of decreased intracellular Ca 2+ medications dogs can take asacol 800 mg on line. The decrease in intracellular Ca2+ is due to a gradual inactivation of Ca2+ channels. It can be short-term, or it can be prolonged if exposure to the benign stimulus is repeated many times. Sensitization Sensitization is the prolonged occurrence of augmented postsynaptic responses after a stimulus to which an animal has become habituated is paired once or several times with a noxious stimulus. At least in the sea snail Aplysia, the noxious stimulus causes discharge of serotonergic neurons that end on the presynaptic endings of sensory neurons. Sensitization may occur as a transient response, or if it is reinforced by additional pairings of the noxious stimulus and the initial stimulus, it can exhibit features of short-term or long-term memory. The long-term potentiation also involves protein synthesis and growth of the presynaptic and postsynaptic neurons and their connections. It resembles posttetanic potentiation but is much more prolonged and can last for days. Unlike posttetanic potentiation, it is initiated by an increase in intracellular Ca2+ in the postsynaptic rather than the presynaptic neuron. It occurs in many parts of the nervous system but has been studied in greatest detail in the hippocampus. It is also postulated that a chemical signal passes from the postsynaptic to the presynaptic neuron, producing a long-term quantal release of glutamate upon afferent stimulation. The end-feet contain many small, clear vesicles that contain acetylcholine, the transmitter at these junctions. The endings fit into depressions in the motor endplate, the thickened portion of the muscle membrane of the junction. Underneath the nerve ending, the muscle membrane of the endplate is thrown into junctional folds. The space between the nerve and the thickened muscle membrane is comparable to the synaptic cleft at synapses. Only one nerve fiber ends on each endplate, with no convergence of multiple inputs. Sequence of Events During Transmission the events occurring during transmission of impulses from the motor nerve to the muscle (see Table 3-2) are somewhat similar to those occurring at other synapses. The impulse arriving in the end of the motor neuron increases the permeability of its endings to Ca 2+. Ca2+ enters the endings and triggers a marked increase in exocytosis of the acetylcholine-containing vesicles. The acetylcholine diffuses to the muscle type nicotinic acetylcholine receptors (Figure 4-18), which are concentrated at the tops of the junctional folds of the membrane of the motor endplate. Binding of acetylcholine to these receptors increases the Na+ and K+ conductance of the membrane, and the resultant influx of Na+ produces a depolarizing potential, the endplate potential. The current sink created by this local potential depolarizes the adjacent muscle membrane to its firing level. Acetylcholine is then removed from the synaptic cleft by acetylcholinesterase, which is present in high concentration at the neuromuscular junction. Action potentials are generated on either side of the endplate and are conducted away from the endplate in both directions along the muscle fiber. The muscle action potential, in turn, initiates muscle contraction, as described in Chapter 3. Endplate Potential An average human endplate contains about 15-40 million acetylcholine receptors. Each nerve impulse releases about 60 acetylcholine vesicles, and each vesicle contains about 10,000 molecules of the neurotransmitter.

The condition is not unique to hemorrhagic shock but occurs in other forms as well symptoms cervical cancer asacol 400mg for sale. It used to be called irreversible shock medications prescribed for anxiety cheap asacol 800mg free shipping, and patients still do die despite vigorous treatment treatment neuroleptic malignant syndrome buy asacol without prescription. However medicine yoga order asacol with american express, more and more patients are saved as understanding of the pathophysiologic mechanisms increases and treatment is improved. Spasm of the precapillary sphincters and venules, especially in the splanchnic region, is a prominent feature at this stage. The reduced capillary perfusion due to the constriction of the precapillary sphincters leads to hypoxic tissue damage. After 3-5 hours, the precapillary sphincters dilate while the venules remain constricted. Blood now enters the capillaries but stagnates in these vessels, so that the tissue hypoxia continues. Capillary hydrostatic pressure rises, and fluid leaves the vascular system in increasing amounts. Granulocytes adhere to the injured vessel walls and release free radicals, especially O 2-, and this causes further tissue damage. An antibody to the protein complex that binds neutrophils to tissue has been reported to improve survival in severe shock. There is evidence that damage to the gastrointestinal mucosa permits entry of bacteria into the circulation. Various positive feedback mechanisms contribute to the production of refractory shock. For example, severe cerebral ischemia leads eventually to depression of the vasomotor and cardiac areas of the brain, causing vasodilation and reduction of the heart rate. These both make the blood pressure drop further, with a further reduction in cerebral blood flow and further depression of the vasomotor and cardiac areas. Another important example of this type of positive feedback is myocardial depression. In severe shock, the coronary blood flow is reduced because of the hypotension and tachycardia (see Chapter 32), even though the coronary vessels are dilated. The myocardial failure makes the shock and the acidosis worse, and this in turn leads to further depression of myocardial function. If the reduction is marked and prolonged, the myocardium may be damaged to the point where cardiac output cannot be restored to normal in spite of reexpansion of the blood volume. This syndrome is characterized by acute respiratory failure with a high mortality, and it can be triggered not only by shock but also by sepsis, lung contusion, other forms of trauma, and other serious conditions. The common feature seems to be damage to capillary endothelial cells and alveolar epithelial cells, with release of cytokines. Other Forms of Hypovolemic Shock Traumatic shock develops when there is severe damage to muscle and bone. This is the type of shock seen in battle casualties and automobile accident victims. Frank bleeding into the injured areas is the principal cause of the shock, although some plasma also enters the tissue. The amount of blood which can be lost into an injury that appears relatively minor is remarkable; the thigh muscles can accommodate 1 L of extravasated blood, for example, with an increase in the diameter of the thigh of only 1 cm. Breakdown of skeletal muscle (rhabdomyolysis) is a serious additional problem when shock is accompanied by extensive muscle crushing (crush syndrome). When pressure on the tissues is relieved and they are once again perfused with blood, free radicals are generated, and these cause further tissue destruction (reperfusion-induced injury). Many of the free radicals are generated because during ischemia, tissue xanthine dehydrogenase is converted to xanthine oxidase, and when perfusion is restored, this enzyme generates O 2-. The xanthine oxidase inhibitor allopurinol and antibodies that prevent neutrophil adhesion reduce the severity of reperfusion injury. An additional cause of tissue damage in reperfused areas is marked intracellular Ca 2+ excess, which is presumably due to exchange of excess intracellular Na + in damaged tissues for extracellular Ca2+.
Note that at about 0 mV the Na+ flux is exactly balanced by an opposite K+ flux medicine neurontin order asacol no prescription, resulting in no net current flow treatment of lyme disease order asacol 800mg without a prescription, and hence no change in the membrane potential medicine you can take while breastfeeding asacol 800 mg overnight delivery. The general rule treatment 1st 2nd degree burns order genuine asacol line, then, is that Synaptic Transmission 121 the action of a transmitter drives the postsynaptic membrane potential toward Erev for the particular ion channels being activated. Although this discussion has focused on the neuromuscular junction, similar mechanisms generate postsynaptic responses at all chemical synapses. The general principle is that transmitter binding to postsynaptic receptors produces a postsynaptic conductance change as ion channels are opened (or sometimes closed). The postsynaptic conductance is increased if-as at the neuromuscular junction-channels are opened, and decreased if channels are closed. However, still other synapses actually decrease the probability that the postsynaptic cell will generate an action potential. Given that most neurons receive inputs from both excitatory and inhibitory synapses, it is important to understand more precisely the mechanisms that determine whether a particular synapse excites or inhibits its postsynaptic partner. The principles of excitation just described for the neuromuscular junction are pertinent to all excitatory synapses. The principles of postsynaptic inhibition are much the same as for excitation, and are also quite general. In both cases, neurotransmitters binding to receptors open or close ion channels in the postsynaptic cell. When these glutamate receptors are activated, both Na+ and K+ flow across the postsynaptic membrane, yielding an Erev of approximately 0 mV for the resulting postsynaptic current. While activation of either one of the excitatory synapses alone (E1 or E2 in Figure 5. Whether the sum of active synaptic inputs results in the production of an action potential depends on the balance between excitation and inhibition. Conversely, if inhibition prevails, then the postsynaptic cell will remain silent. Summation is therefore a neurotransmitterinduced tug-of-war between all excitatory and inhibitory postsynaptic currents; the outcome of the contest determines whether or not a postsynaptic neuron fires an action potential and, thereby, becomes an active element in the neural circuits to which it belongs (Figure 5. Two Families of Postsynaptic Receptors the opening or closing of postsynaptic ion channels is accomplished in different ways by two broad families of receptor proteins. The receptors in one family-called ionotropic receptors-are linked directly to ion channels (the Greek tropos means to move in response to a stimulus). These receptors contain two functional domains: an extracellular site that binds neurotransmitters, and a membrane-spanning domain that forms an ion channel (Figure 5. Thus ionotropic receptors combine transmitter-binding and channel functions into a single molecular entity (they are also called ligand-gated ion channels to reflect this concatenation). Such receptors are multimers made up of at least four or five individual protein subunits, each of which contributes to the pore of the ion channel. The second family of neurotransmitter receptors are the metabotropic receptors, so called because the eventual movement of ions through a channel depends on one or more metabolic steps. These receptors do not have ion channels as part of their structure; instead, they affect channels by the activation of intermediate molecules called G-proteins (Figure 5. For this reason, metabotropic receptors are also called G-protein-coupled receptors. Metabotropic receptors are monomeric proteins with an extracellular domain that contains a neurotransmitter binding site and an intracellular domain that binds to G-proteins. Neurotransmitter binding to metabotropic receptors activates G-proteins, which then dissociate from the receptor and interact directly with ion channels or bind to other effector proteins, such as enzymes, that make intracellular messengers that open or close ion channels. Thus, G-proteins can be thought of as transducers that couple neurotransmitter binding to the regulation of postsynaptic ion channels. The postsynaptic signaling events initiated by metabotropic receptors are taken up in detail in Chapter 7. Neurotransmitter release at all presynaptic terminals on a cell results in receptor binding, which causes the opening or closing of specific ion channels. The resulting conductance change causes current to flow, which may change the membrane potential.
Cheap asacol generic. How to diagnose pneumonia in young children? | Symptoms of Pneumonia in Children | Dharani Health Tv.