"Order genuine chloromycetin, medications you can crush".
By: Q. Marik, M.S., Ph.D.
Professor, New York University Long Island School of Medicine
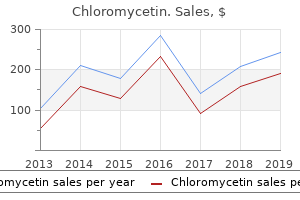
Weekly meetings are held to discuss evaluation results medications 2355 cheap chloromycetin master card, determine eligibility and identify concerning issues before a patient is scheduled medications qid cheap 250 mg chloromycetin mastercard. Once treatment begins the hematologist provides the majority of care with the multidisciplinary team on hand for consults treatment uti discount 250mg chloromycetin with amex. Patients are seen in the clinic daily 5 medications that affect heart rate buy 250 mg chloromycetin with amex, staying the better portion of the day, synonymous to that of a day hospital. Patient rounds include toxicity evaluations, physical exams, medication review and reinforcement of the treatment plan. Instructions are provided describing expected toxicities, symptom management, medications and emergency instructions. Prophylactic antiemetics, antimicrobials and growth factors are used as part of supportive care. Both are reviewed annually for revisions based on current evidence and program experience with a mechanism to document any deviations. Patient/carer group completed the draft tool then attended a focus group interview where each item was further discussed to gain consensus. Clinicians participated in an online survey of the tool scoring each item for relevance followed by a group tele-conference where consensus on content was obtained. Properties of feasibility, acceptability and validity are being tested in a larger multi-centre cross sectional study. A second discrete choice study evaluated patient preferences (3), and 3 others evaluated patient preferences and value mapping (5-7). It observes life satisfaction, including everything from physical health, family, education, employment, wealth, religious beliefs, finance and the environment. Quality of life screening is not done, or the measurement necessary for eligibility to enroll on a clinical trial or to start a new conventional therapy this was a pilot project of 538 Abstracts screening patients and their caregivers for quality of life. The goal was to identify areas that oncology clinicians could better assist and care for multiple myeloma patients and their caregivers. Many quality of life studies have been done in oncology, but none in multiple myeloma specifically, involving both patient and their caregiver. Many patients are living with significant side effects and disabilities requiring assistance from caregivers and equipment. Process: the purpose of the pilot was described to patients and their caregivers both verbally and with a written letter attached to each survey. Questionnaires were on paper, they were provided a clipboard, pencil and an envelope to seal the questionnaire when it was completed. It was noted that approximately 40-66% of patients complained of: lack of energy, easily fatigued, trouble walking because of pain and emotional ups and downs. The contrast to this is that caregivers complained 60-83% of increased level of stress, fear that their loved one will die and feeling upset to see their loved on deteriorate. This pilot project opened communication with patients, their caregivers and healthcare providers. Subjects completed their surveys independently but then were able to talk about it and other related topics that prior to this might have been uncomfortable. Of these, 33% of patients who are diagnosed are living more than 10 years with a further 47% surviving 5 years or more (1). Gold standard treatment as approved by for induction or first relapse therapy is a bortezomib based regime. This can mean weekly or twice-weekly trips to the local hospital to receive their treatment (2). The Myeloma team of the University Hospital of Wales aimed to introduce self-administration of bortezomib to give patients more control of their treatment. Being able to offer fewer visits to the hospital and encouraging a patient to take control of their treatment is a step forward for the team in Cardiff. Our review showed patients spent around 2 hours at the hospital for bortezomib treatment.
The need for diagnostic certainty rarely requires surgical exploration of the plexus treatment h pylori order chloromycetin 500mg visa. Clinical pictures Acute encephalopathy Neurological complications of chemotherapy Neurotoxicity of antineoplastic drugs is frequent (Table 2) symptoms your dog has worms order chloromycetin 500 mg with mastercard. As for radiation-induced complications treatment 247 discount chloromycetin 250 mg line, a low therapeutic index is an important dose-limiting factor for these agents treatment genital herpes generic chloromycetin 250mg visa. Chemotherapy neurotoxicity produces a limited number of nonspecific clinical pictures [58]. Neuropathy lowed by a state of confusion that may be associated either with stupor or, more often, with agitation. They are typically characterized by the acute onset of encephalopathy with fluctuating motor deficit that resolves spontaneously. Chronic encephalopathy the most characteristic is a "subcortical dementia" of variable severity developing progressively, months to years after treatment that often but not always included a combination of cranial radiotherapy and chemotherapy. The syndrome is characterized by apathy, intellectual and memory loss, frontal syndrome, sleep disorders and often incontinence and gait disorders. Spontaneous improvement may occur but, in many cases, progressive deterioration is the rule. This syndrome is seen with suramin, an agent used for prostate cancer [20], and sometimes after Ara-C. Loss of position sense and ataxia are frequent in cisplatin-induced neuropathy, whereas taxane-induced neuropathy affects preferentially pinprick and tact. Peripheral neuropathy this disorder follows doses of cisplatin of more than 400 mg/m2 and is characterized by numbness and tingling in the extremities, which are occasionally painful. It affects predominantly large sensory fibres; the deep tendon reflexes disappear, and patients lose proprioception, sometimes to the point where they cannot walk. However, pinprick and temperature appreciation are relatively spared, and motor power may be entirely normal. If the patient survives the cancer, the neuropathy may improve and even return to normal after many months [58, 64]. Ototoxicity this is sometimes associated with a vestibulopathy and is another frequent complication of cisplatin. Hearing loss, resulting from hair cell damage, is often subclinical, detected only by serial audiograms; most loss occurs in the high-frequency range. Cranial nerve neuropathies these have occasionally been reported after infusion of cisplatin into the internal carotid artery [1]. After intracarotid treatment, the disorder is sometimes heralded by seizures and generally characterized by slowly progressive neurological dysfunction. The pathology is that of a necrotizing encephalopathy, giving an appearance similar to that of radiation damage, but strictly confined to the vascular territories perfused by the drug. Ifosfamide Ifosfamide is an analogue of cyclophosphamide with substantial neurotoxicity. Thiotepa this drug is not neurotoxic when it is given systemically at conventional doses. At high doses prior to bone marrow transplantation, severe neurotoxicity may occur (somnolence, seizures, coma and even death) [49]. Procarbazine Procarbazine is now always given orally; it may produce an encephalopathy ranging from mild drowsiness to stupor or, rarely, a manic psychosis. A peripheral neuropathy occurs in some patients after several weeks of treatment; it is reversible after discontinuation of the drug [81]. Vincristine Vincristine and, to a lesser degree, vinblastine and vindesine cause peripheral neuropathy. Most patients receiving vincristine develop paraesthesias in the fingertips and feet, and absent ankle jerks. In a few patients, there may be loss of all sensory modalities as well as motor weakness and, in particular, bilateral footdrop. The weakness 702 can begin several weeks after completion of the course of vincristine. The drug should be given with care to patients with any preexisting peripheral neuropathy.
Expression of the nonclassical gene products is limited to certain specific cell types treatment ulcerative colitis order chloromycetin us. Although functions are not known for all of these gene products symptoms ulcer generic 500 mg chloromycetin with mastercard, some may have highly specialized roles in immunity treatment solutions quality chloromycetin 500mg. For this reason treatment 1st degree burn cheap chloromycetin 500 mg line, most individuals inherit the alleles encoded by these closely linked loci as two sets, one from each parent. An individual inherits one haplotype from the mother and one haplotype from the father. The alleles are codominantly expressed; that is, both maternal and paternal gene products are expressed in the same cells. If mice are inbred (that is, have identical alleles at all loci), each H-2 locus will be homozygous because the maternal and paternal haplotypes are identical, and all offspring therefore express identical haplotypes. These designations refer to the entire set of inherited H-2 alleles within a strain without having to list each allele individually (Table 7-1). For example, if an H-2b strain is crossed with an H-2k, then the F1 inherits both parental sets of alleles and is said to be H-2b/k (Figure 7-2a). In an outbred population, each individual is generally heterozygous at each locus. When the father and mother have different haplotypes, as in the example shown (Figure 7-2c) there is a one-in-four chance that siblings will inherit the same paternal and maternal haplotypes and therefore be histocompatible with each other; none of the offspring will be histocompatible with the parents. B, which has the genetic background of parental strain A but the H-2 complex of strain B. Crossing inbred strain A (H-2a) with strain B (H-2b) generates F1 progeny that are heterozygous (a/b) at all H-2 loci. The F1 progeny are interbred to produce an F2 generation, which includes a/a, a/b, and b/b individuals. The F2 progeny homozygous for the B-strain H-2 complex are selected by their ability to reject a skin graft from strain A; any progeny that accept an A-strain graft are eliminated from future breeding. The selected b/b homozygous mice are then backcrossed to strain A; the resulting progeny are again interbred and their offspring are again selected for b/b homozygosity at the H-2 complex. This process of backcrossing to strain A, intercrossing, and selection for ability to reject an A-strain graft is repeated for at least 12 generations. In this way A-strain homozygosity is restored at all loci except the H-2 locus, which is homozygous for the B strain. Any phenotypic differences that can be detected between congenic strains are related to the genetic region that distinguishes the strains. Figure 7-3 outlines the steps by which the H-2 complex of homozygous strain B can be introduced into the background genes of homozygous strain A to generate a congenic strain, denoted A. During production of congenic mouse strains, a crossover event sometimes occurs within the H-2 complex, yielding a recombinant strain that differs from the parental strains or the congenic strain at one or a few loci within the H-2 complex. Figure 7-4 depicts haplotypes present in several recombinant congenic strains that were obtained during pro- H-2 loci Strain Parental Congenic Recombinant congenic A B10 B10. Crossover events within the H-2 complex produce recombinant strains, which have a-haplotype alleles (blue) at some H-2 loci and b-haplotype alleles (orange) at other loci. Association of the chain with 2-microglobulin is required for expression of class I molecules on cell membranes. The chain is anchored in the plasma membrane by its hydrophobic transmembrane segment and hydrophilic cytoplasmic tail. The 2-microglobulin is similar in size and organization to the 3 domain; it does not contain a transmembrane region and is noncovalently bound to the class I glycoprotein. Both types of membrane glycoproteins function as highly specialized antigen-presenting molecules that form unusually stable complexes with antigenic peptides, displaying them on the cell surface for recognition by T cells. The enzyme papain cleaves the chain just 13 residues proximal to its transmembrane domain, releasing the extracellular portion of the molecule, consisting of 1, 2, 3, and 2-microglobulin. Purification and crystallization of the extracellular portion revealed two pairs of interacting domains: a membrane-distal pair made up of the 1 and 2 domains and a membrane-proximal pair composed of the 3 domain and 2-microglobulin (Figure 7-6a).
If the cell remains self-reactive treatment centers cheap 250 mg chloromycetin amex, it may be rescued by another cycle of rearrangement treatment urinary tract infection buy generic chloromycetin 250 mg on-line, but if it continues to react strongly with self it will undergo programmed cell death or apoptosis and be deleted from the repertoire (clonal deletion; bottom left panel) treatment 4 burns order 250 mg chloromycetin with amex. This antigen-induced loss of cells from the B-cell population is known as clonal deletion medicine wheel native american purchase chloromycetin 500 mg visa. If the transgenic mouse does not express H-2Kb, normal numbers of B cells develop, all bearing transgene-encoded anti-H-2Kb receptors. However, in mice expressing both H-2Kb and the immuno-globulin transgenes, B-cell development is blocked. Normal numbers of pre-B cells and immature B cells are found, but B cells expressing the anti-H-2Kb immunoglobulin as sIgM never mature to populate the spleen and lymph nodes; instead, most of these immature B cells die in the bone marrow by apoptosis. This is because the anti-H-2Kb immunoglobulin on the immature B cells interacts strongly with the H-2Kb molecules on the bone marrow stromal cells. Closer analysis of this experimental system and others like it revealed the surprising finding that clonal deletion was not the only outcome in these circumstances. There was, in fact, an interval before cell death during which the selfreactive B cell might be rescued by further gene rearrangements that replaced the self-reactive receptor with a new receptor that was not autoreactive. This mechanism for replacing receptors, termed receptor editing, works as follows. As a consequence of the continued presence of recombinase, light-chain gene rearrangement continues, even though the cell has already made one productive rearrangement at this locus. The light-chain loci are able to make numerous successive rearrangements. This continuation of light-chain gene rearrangement has parallels with the continuation of -gene rearrangement in developing T cells, but it should be emphasized that in B cells it only occurs if the receptor encounters a strongly cross-linking antigen. More recently, receptor editing has been shown unambiguously in mice bearing transgenes for autoantibody heavy and light chains that have been placed within the immunoglobulin loci by the homologous recombination method explained in Appendix I, Section A-47. The transgene imitates a primary gene rearrangement and is surrounded by unused endogenous gene segments. In mice that express the antigen recognized by the transgene-encoded receptor, the few mature B cells that emerge into the periphery have used these surrounding gene segments for further rearrangements that replace the autoreactive light-chain transgene with a nonautoreactive rearranged gene. At a light-chain locus, the multiplicity of V and J segments allows the unused V and J gene segments to be selected for multiple further rearrangements. There are no available D segments at a rearranged heavy-chain locus, so a new rearrangement cannot simply occur by the normal mechanism and at the same time remove the preexisting one. This has been observed in some B-cell tumors, but whether it occurs during normal B-cell development in response to signals from autoreactive B-cell receptors is not known. It was originally thought that successful production of a heavy chain and a light chain caused the almost instantaneous shut down of further light-chain locus rearrangement and that this ensured both allelic and isotypic exclusion (see Section 7-10). The unexpected ability of self-reactive B cells to continue to rearrange their light-chain genes, even after having made a productive rearrangement, has raised questions about this supposed mechanism of allelic exclusion. Furthermore, any additional productive rearrangement that did still occur would not necessarily breach allelic exclusion: if it occurred on the same chromosome it would eliminate the existing productive rearrangement, while if it occurred on the other chromosome it would be nonproductive in two out of three cases. Consistent with this idea, it appears that allelic exclusion is not absolute, since there are rare B cells that express two light chains. We have so far discussed the fate of newly formed B cells that undergo multivalent cross-linking of their sIgM. Those immature B cells that encounter more weakly cross-linking self antigens of low valence, such as small soluble proteins, respond differently. In this situation, the self-reactive B cells tend to be inactivated and enter a state of permanent unresponsiveness, or anergy, but do not immediately die. Anergic B cells cannot be activated by their specific antigen even with help from antigen-specific T cells (see Section 1-15). The anergic cells retain their IgM within the cell and transport little to the surface. It seems that signal transduction is blocked at a step before the phosphorylation of the Ig and Ig chains (see Section 6-6), although the exact step is not yet known. The signaling defect may involve the inability of B-cell receptor molecules on tolerant B cells to enter regions of the cell in which important other signaling molecules normally segregate in order to transmit a complete signal subsequent to antigen binding.
It seems likely that these regulatory proteins and others like them together direct the developmental program of Blineage cells symptoms 0f parkinson disease buy chloromycetin 500mg amex. In particular medications 1 gram chloromycetin 250 mg low price, the proteins involved in the tissue-specific transcriptional regulation of immunoglobulin genes are likely to be important in regulating the order of events in gene rearrangement treatment medical abbreviation cheap chloromycetin 250 mg fast delivery. Yet rearrangements of T-cell receptor genes do not occur in B-lineage cells symptoms emphysema safe 500 mg chloromycetin, nor do complete rearrangements of immunoglobulin genes occur in T cells. The ordered rearrangement events that do occur are associated with low-level transcription of the gene segments about to be joined. Second panel: in the early pro-B cell, lineage-specific proteins bind to the Ig enhancer elements (e); for the heavy-chain locus these are in the J-C intron and 3 to the C exons. Third panel: the rearrangement of D to J that follows the initiation of transcription of the D and J gene segments leads to a low level of transcription from promoters located upstream of the D gene segments. For some D-J joins in the mouse this may result in the expression of a truncated heavy-chain (D) at levels sufficient to abort further development, but in most cases it is followed by initiation of low-level transcription of an upstream V gene segment. As a consequence of immunoglobulin gene rearrangement, the promoter upstream of the V gene segments is brought nearer to the enhancers associated with the C gene segments. This in turn brings transcription factors that have bound the promoter and enhancer into proximity, resulting in a dramatic increase in transcription of the rearranged segments. Thus, gene rearrangement can be viewed as a powerful mechanism for regulating gene expression, as well as for generating receptor diversity. Several cases of gene rearrangement that brings the rearranged genes under the control of a new promoter are known from prokaryotes and single-celled eukaryotes, but in vertebrates only the immunoglobulin and T-cell receptor genes are known to use gene rearrangement to regulate gene expression. T cells in the thymus undergo a series of gene segment rearrangements similar to those of B cells. They must assemble a functional gene for each Tcell receptor chain while at the same time ensuring that each T cell expresses receptors of only one specificity. Not surprisingly, T cells follow an almost identical strategy to B cells, in that the receptor is assembled in stages, with each stage being checked for correct assembly. Moreover, as in B cells, a productively rearranged gene is expressed as soon as it is made, and the product(s) are assembled into a receptor complex, in this case either a pre-T-cell receptor or a bona fide T-cell receptor. Expression of this receptor is instrumental in promoting further development, which ultimately results in shutting down further rearrangement at the locus that has just been active. Despite the similarities with B-cell development, the control of antigen-receptor assembly during development is more complicated for T cells because there are two different kinds of T cells that could be generated from an undifferentiated precursor: T cells or: T cells. These two types are distinguished by the different genetic loci that are used to make their T-cell receptors, as described in Section 4-13. Thus, the T-cell developmental program must control to which of the two lineages a precursor commits and must also ensure that a fully developed T cell only expresses receptor components of one or the other lineage. Another key difference between B and T cells is that the final assembly of an immunoglobulin leads to cessation of gene rearrangement and initiates the further differentiation of the B cell, whereas in the case of T cells, rearrangement of the V gene segments continues unless there is signaling to positively select the receptor. The two types of T cell also differ in function, although relatively little is known about the function of: T cells (see Sections 2-28 and 3-19). The gene rearrangements found in thymocytes and in mature: and: T cells suggest that these two cell lineages diverge from a common precursor after certain gene rearrangements have already occurred. Mature: T cells can have productively rearranged -chain genes, and mature: T cells often contain rearranged, but mostly (about 80%) out-of-frame, -chain genes. At this stage, if the thymocyte receives signals through the: receptor, the cell commits to the: lineage, switching off expression of the -chain gene and thus the pre-T receptor (middle left panel). This cell then matures into a: T cell and migrates out of the thymus into the peripheral circulation (bottom left panel). The, and loci undergo rearrangement almost simultaneously in developing thymocytes. At present, the factors that regulate the lineage commitment of these cells are not known; indeed, commitment to the: lineage might simply depend on whether productive rearrangements at a and a gene have occurred in the same cell. In this view, successful rearrangement of a and a gene leads to the expression of a functional: T-cell receptor that signals the cell to differentiate along the: lineage.
Discount chloromycetin 250 mg with mastercard. Colds Flu and Antibiotics.